The Power of Caffeine
Here's what Michael Pollan Learned after Quitting Caffeine for 3 Months. Informative and entertaining interview with Joe Rogan.

Here's what Michael Pollan Learned after Quitting Caffeine for 3 Months. Informative and entertaining interview with Joe Rogan.
Full disclosure: I have been doubly vaccinated with the Modern Vaccine. I have trusted ubiquitous assertions by government and health care providers, that the vaccines are safe. I knew that the vaccines were extraordinary quick to market. I wondered about their safety, but I considered the COVID virus itself to be a much greater risk. I am extremely concerned about the existence of COVID and the devastation it has caused, medical and economic. I am extremely concerned about the potential emergence of variants and COVID.
Also, I have long been suspicious about the effects of tribal affinities on the free flow of information (on many topics). On topics related to the pandemic, there have been major reversals by medical authorities in the past 1 1/2 years that concern me. Some of these relate to the alleged efficacy (and non-efficacy) of mask-wearing, where government mandates were issued in the absence of controlled studies. I am also aware that we have seen very little in the way of data regarding adverse side effects regarding the general population, as well as populations of adolescents and immune-compromised and pregnant individuals. It is also apparent that the misinformation relating to the wearing of masks could be motivated by an inclination to downplay vaccine-related deaths (in order to encourage people to get the vaccines on a nationwide basis).
It is in this context that I am sharing the following materials. I have no medical expertise. I find the following information intriguing. I hope that this information (which has possibly been suppressed) is further developed in the public sphere. Here is the basis for my concerns, a discussion hosted by Brett Weinstein, who has a long history of fearlessly discussing topics that run counter "preferred" public narratives.
The guests suggest that we need an honest conversation regarding use of the the COVID vaccines regarding certain populations where there is natural immunity (children, young teenagers and those who have already had COVID) and where there is alarming data (pregnant women). They also advocate that we badly need honest national dialogue regarding the promising data based on the prophylactic use of repurposed Ivermectin.
Here are two key points made during this deeply engaging discussion:
Point 1. An ongoing course of Ivermectin, long-shown to be a safe drug, is fantastically effective in protecting people from COVID. Brett notes that he and his wife Heather were not vaccinated, but have chosen to use Ivermectin prophylactically. Brett and the guests argue that where a safe alternative to the vaccines is available, this information should be available. The guests are convinced, based on discussed evidence, that Ivermectin is a potentially a "miracle drug" that should be widely repurposed and made available to the public. They are gravely concerned that discussions regarding Ivermectin have been suppressed on the Internet, for social and financial motives they discuss.
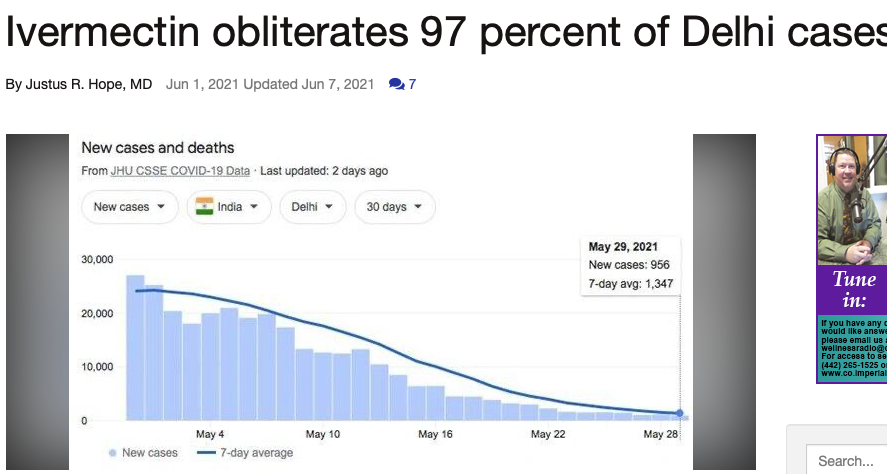
Today, I spotted these graphs regarding Ivermectin usage in India. I cannot vouch for the accuracy of the information in this June 1, 2021 article by Justus R. Hope, a doctor, but it is eye-popping and compels me to know more:
Another excerpt from this article:
A 97% decline in Delhi cases with Ivermectin is decisive - period. It represents the last word in an epic struggle to save lives and preserve human rights. This graph symbolizes the victory of reason over corruption, good over evil, and right over wrong. It is as significant as David’s victory over Goliath. It is an absolute vindication of Ivermectin and early outpatient treatment. It is a clear refutation of the WHO, FDA, NIH, and CDC's policies of "wait at home until you turn blue" before you get treatment.
Point 2. On the vaccine side, the guests express concern that there are significant adverse side-effects to the COVID vaccines that are not being discussed widely. In fact, the information is being suppressed, the group strongly suggests, because it doesn't fit the ongoing narrative that the COVID vaccines are "safe." Further, the data regarding adverse side effects is not systematically being collected, much less discussed. The conversation suggests that the VAERS database (voluntary reports) significantly under-reports incidents. Data suggest that the rate of deaths so far from the COVID vaccines in the U.S. might be in the range of 5,000-20,000, the lower end which is greater than the number of deaths from all other vaccines in the U.S. over the past 70 years. For further information on this point, consider Steve Kirsch's recent article at TrialSiteNews, where you will see many details on which he based his concerns in the above video: "Should You Get Vaccinated." The guests also argue that silicon valley is actively suppressing youtube videos and other information. Adverse vaccine-related bloodwork seems to resemble the bloodwork of those who have COVID. The biggest alarm here, the guests agree, is the lack of an alarm.
Here are a few excerpts:
However, based on what I now know about the vaccine side effects, current COVID rates, and the success rate of early treatment protocols, the answer I would give today to anyone asking me for advice as to whether to take any of the current vaccines would be, “Just say NO.”
The current vaccines are particularly contraindicated if you have already been infected with COVID or are under age 20. For these people, I would say “NO! NO! NO!”In this article, I will explain what I have learned since I was vaccinated that totally changed my mind. You will learn how these vaccines work and the shortcuts that led to the mistakes that were made. You will understand why there are so many side effects and why these are so varied and why they usually happen within 30 days of vaccination. You will understand why kids are having heart issues (for which there is no treatment), and temporarily losing their sight, and ability to talk. You will understand why as many as 3% may be severely disabled by the vaccine.
What I find deeply disturbing is the lack of transparency on how dangerous the current COVID vaccines are. Healthy people could end up dead or permanently disabled at a rate that is “off the charts” compared with any other vaccine in our history. Look at the death report in our government’s official Vaccine Adverse Event Reporting System (VAERS) summarized in the tweet below. This is the most deadly vaccine we’ve ever made by a long shot. That’s why they have to give you incentives to get vaccinated. They need to vaccinate everyone BEFORE people read this article or watch this video of Dr. Peter McCullough explaining clearly why the current COVID vaccines are unsafe and completely unnecessary for our children.
Kirsch expresses special concerns with the risks of the COVID vaccines for pregnant women:
82% miscarriage rate in first 20 weeks (10% is the normal rate). It is baffling that the CDC says the vaccine is safe for pregnant women when it is so clear that this is not the case. For example, one our family friends is a victim of this. She miscarried at 25 weeks and is having an abortion on 6/9/21. She had her first shot 7 weeks ago, and her second shot 4 weeks ago. The baby had severe bleeding of the brain and other disfigurements. Her gynecologist had never seen anything like that before in her life. They called in a specialist who said it was probably a genetic defect (because everyone buys into the narrative that the vaccine is safe it is always ruled out as a possible cause). No VAERS report. No CDC report. Yet the doctors I’ve talked to say that it is over 99% certain it was the vaccine. The family doesn’t want an autopsy for fear that their daughter will find out it was the vaccine. This is a perfect example of how these horrible side effects just never get reported anywhere.
I invite you to listen to the detailed conversation in the video above. I'm writing this as I watch the live discussion. I will update with more after I finish viewing the entire video . . .
[June 12 2021 two updates]
I love this exchange between Steve Kirsch and hundreds of Youtube Subscribers who told him that they appreciated his passion and his message but warned him that his manners were rude and that he was getting in the way of his own message.

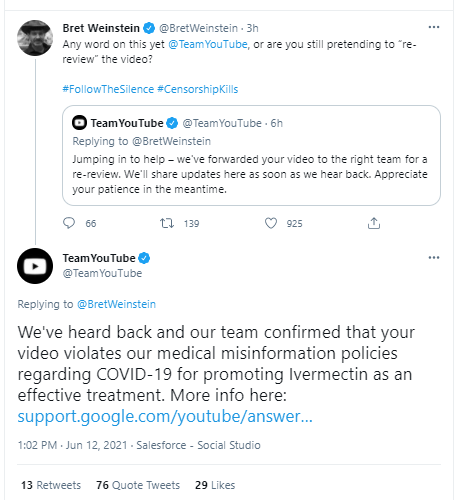
Second, Brett might have sounded paranoid (to those who don't know the abuse that he has suffered at the hands of social media corporations), but here it comes, just as Brett predicted:
From an anonymous Medical Student at American University (an excerpt from a longer article):
IDD64 @IDD64 asks: “What happened to “nobody’s saying sex isn’t real”?”
This is actually what compelled me to speak out about this practice in the first place. Well-intentioned non-medical people often assume that medical schools are teaching something like, “Gender identity can be fluid and varied, but biological sex is real, binary, and relevant in medical contexts.” This idea is around five years out of date in the most progressive of institutions. I have been told multiple times in several classes that biological sex is a social construct – not just gender. Granted, I can speak only for my institution, but this change has been frustrating and disturbing to witness.
Robert Woolley @RandomlyBob asks: “Do any of the required textbooks also avoid using those words? If not, might you ask those professors if they think the books are either inaccurate or offensive?”
Our curriculum is constantly subject to revision. Around two-thirds of our written materials have been updated with this new language. For the one-third that has remained out-of-date, our class has received multiple apologetic, itemized emails from course instructors in which they provide corrections, beg for forgiveness and patience, and avow to “do better”. In class, we have been given multiple histories in which the patient’s sex has been deleted, even for cases involving disorders which can manifest differently between the sexes. The words “female” and “male” are being erased and replaced.
When you arrive at the doctor's office to check in with the receptionist, you are often handed a small pack of paperwork to fill out. Until that moment, you have probably been focused on your own ailment or your own medical worries. Luckily, for most of us--most of the time--our own health concerns will more or less resolve and life will more or less go on.
For all of us, however, that typical pack of doctor office paperwork contains a magic page that has the power to boost our happiness through the roof, if only we employ the correct frame of gratitude. I'm referring to the page that looks something like this:
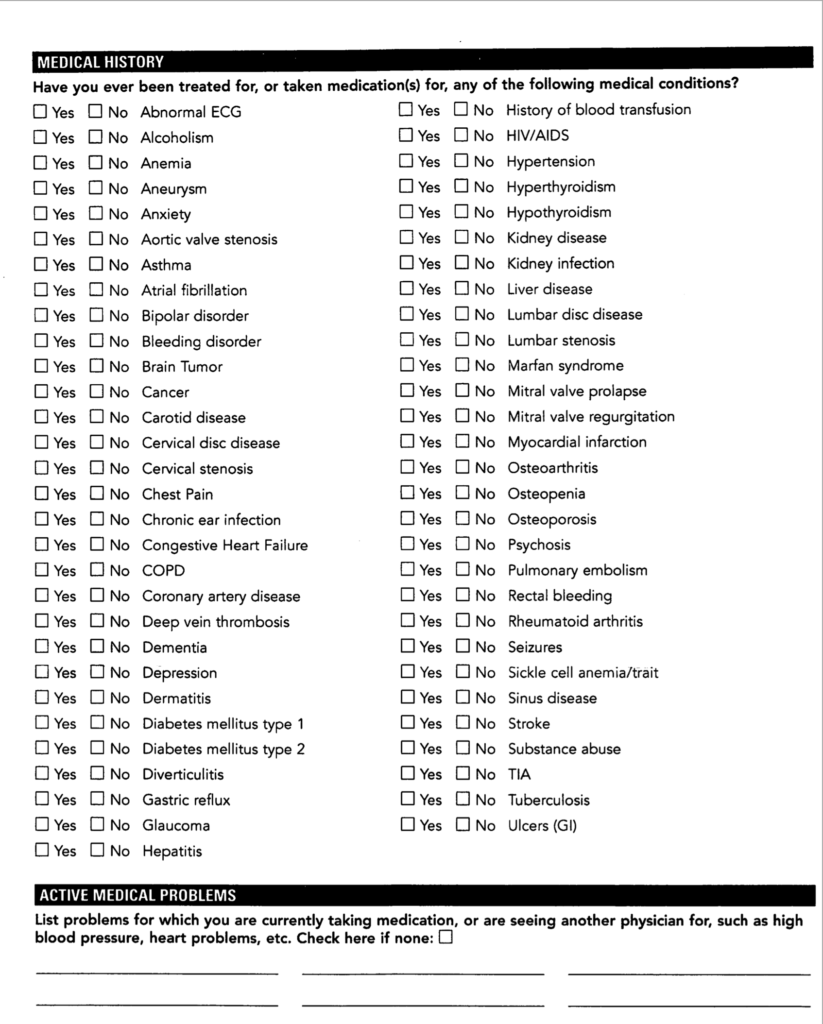
This page gives us the opportunity to breathe a cosmic sigh of relief that we do not have most of those ailments on that list. That's how I try to see it as I check off all most of those boxes with a "no." Thank goodness I don't have most of those medical problems. And this is merely the beginning of what I'm proposing as a journey of gratitude.
Instead of thinking about my own health problem, instead of being frustrated that my own body is not operating perfectly, the above page is a reminder that my body is an extraordinarily complex adaptive system--lots of little parts have self-organized into something so complicated that it seems miraculous. No humans could possibly make a tongue or an eye or a liver as high functioning or as elegant as the natural versions.
Imagine that humans in the distant future worked very hard and came much closer to making a reasonably functioning robotic human. Then imagine their supervisors sending down a new work order to make sure that this robot is also sentient. Imaging the groaning you would hear from the engineering team! Then imagine that the supervisors send down another new work order to make sure that this artificial human could also repair itself if it became damaged! Imaging louder groaning, especially when the supervisors remind the team that this self-repair must respond to hundreds of millions of microscopic threats and do it as well as the human immune system.
Then imagine that the supervisors send down yet another work order advising the team that they must design their human so that it runs on almost anything that it puts in its mouth. Even louder groaning. Mutiny is threatened.
Finally, thousands of years later, when millions more engineers (and their great great great great grand-engineers) have successfully created a passable artificial human, the supervisors call down with one more new request: Make sure that these artificial humans can create tiny artificial humans the size of a pinpoint that will grow, within the body of one of the robots, into large artificial humans who become wise through their interactions with any of dozens of environments. Then imagine all the engineers quitting their jobs.
At the doctor's office, our question should not be "Why doesn't my body work perfectly?" We shouldn't even complain that we sometimes have one or more of those ailments on the long checklist handed to us by the doctor's receptionist. A better question is "How is it possible that the actions of countless individual molecules self-organize into trillions of cells that result in emergent coordinated macroscopic behaviors such as the ability to walk into a doctor's office?" Even more simply, the first question should always be "How is it possible that human bodies work at all, ever?"
Answer not forthcoming.