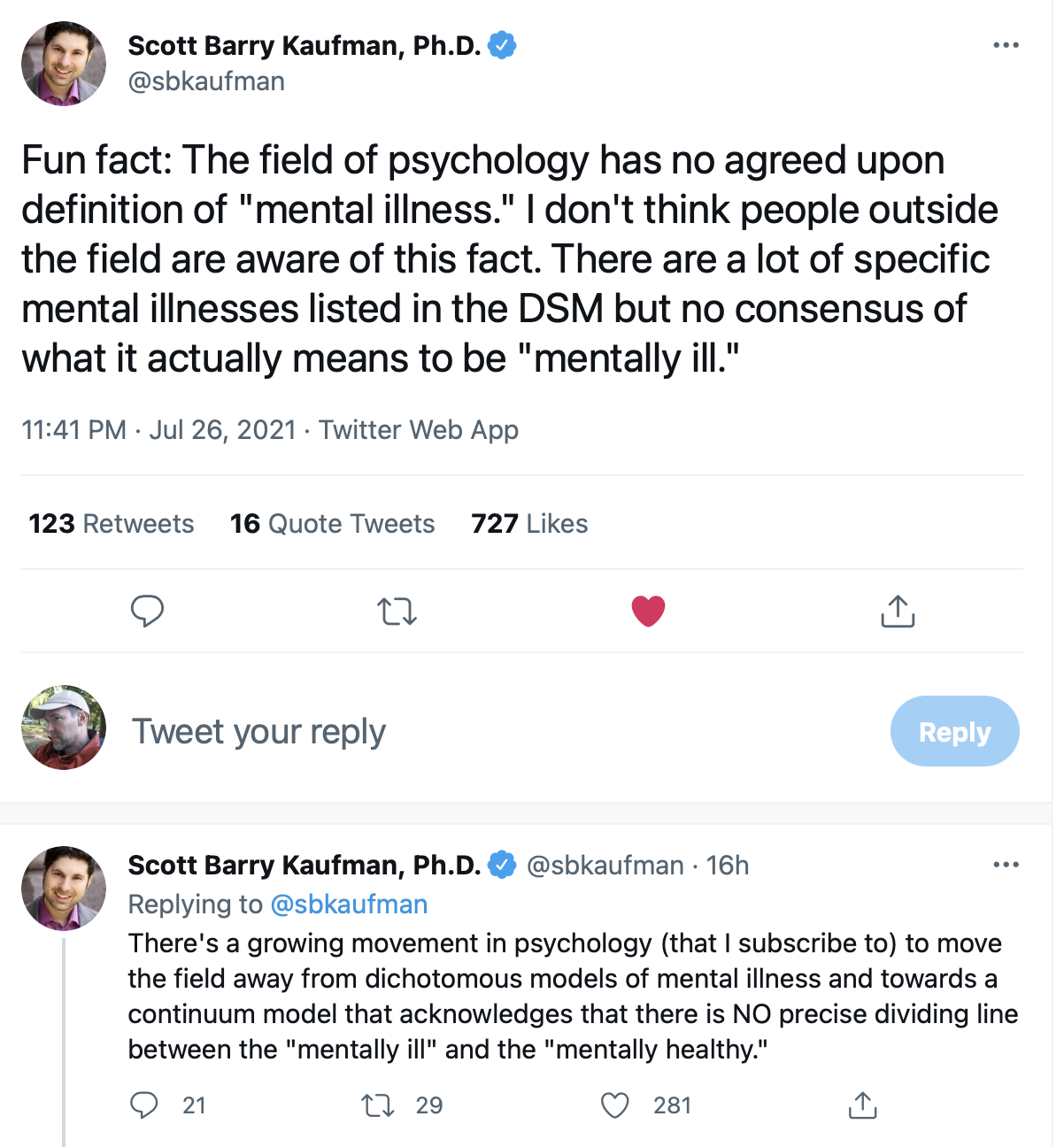
Fascinating. So what is it, at bottom, to call someone "mentally ill? Is it essentially name calling? We are surrounded highly functional people who periodically and temporarily seem highly dysfunctional in specific ways. We have been cobbled together by natural selection, living Rube Goldberg machines, we are also equipped with sophisticated built-in PR departments that make it seem like we are more purposeful, more functional than we actually are. Further, Randolph Nesse has made a strong case that many "mental illnesses" are adaptive. What does it help use a global stamp of "mentally ill"?
The question “What is a mental disorder? ”has been addressed by Jerome Wakefield, a social worker, clinician, researcher, and philosopher at New York University. His pithy conclusion is that mental disorders are characterized by “harmful dysfunction.”“Dysfunction”means a malfunction in a useful system shaped by natural selection. “Harmful”means that the dysfunction causes suffering or other harm to the individual. Wakefield’s analysis grounds psychiatric diagnosis in an evolutionary understanding of the normal functions of brain/mind, the same way the rest of medicine understands pathology in the context of normal physiology. His cogent analysis has, however, had little influence on how psychiatrists make diagnoses.
A new “affirmative care” standard of mental health care has been adopted by nearly every medical accrediting organization. The American Psychological Association guidelines go much further than respecting and supporting trans identities; they mandate that therapists adopt gender ideology themselves. Therapists must accept and affirm the patient’s self-diagnosis. Shrier likens this to telling an anorexic teen “If you think you are fat, then you are. Let’s talk about liposuction and weight-loss programs”. She asks whether a standard guided less by biology than by political correctness is in the best interests of the patient.
We don’t provide affirmative care for anorexia. We don’t say “Yes, you are fat” and offer to help them reduce their weight even more. Part of a therapist’s role is to question a patient’s self-assessment.
Dr. Hall emphasizes that she is open to current treatments, but only where the patient needs them:
I support hormones and gender surgeries for adults who will benefit from them. I care about the welfare of these adolescent girls and it bothers me that some of them may be unduly influenced and take irreversible steps they will later regret.
Dr. Hall concludes:
[Abigail Shrier's book] will undoubtedly be criticized just as Lisa Littman’s study was. Yes, it’s full of anecdotes and horror stories, and we know the plural of anecdote is not data, but Shrier looked diligently for good scientific studies and didn’t find much. And that’s the problem. We desperately need good science, and it’s not likely to happen in the current political climate. Anyone who addresses this subject can expect to be attacked by activists. Is ROGD a legitimate category? We don’t know, since the necessary controlled studies have not been done. I fully expect Shrier to be called a transphobe and to be vilified for harming transgender people, and I’m sure I will be labeled a transphobe just for reviewing her book.
She brings up some alarming facts that desperately need to be looked into. The incidence of teen gender dysphoria is rising and appears to be linked to internet influences and social peer groups. The number of people identifying as lesbians is dropping. Therapists are accepting patients’ self-diagnoses unquestioningly, and irreversible treatments are being offered without therapist involvement. We know at least some of these patients will desist and detransition, and we have no way to predict which ones. Children are being instructed in how to lie to parents and doctors to coerce them into providing the treatments they want. Families are being destroyed.
Full disclosure: I have been doubly vaccinated with the Modern Vaccine. I have trusted ubiquitous assertions by government and health care providers, that the vaccines are safe. I knew that the vaccines were extraordinary quick to market. I wondered about their safety, but I considered the COVID virus itself to be a much greater risk. I am extremely concerned about the existence of COVID and the devastation it has caused, medical and economic. I am extremely concerned about the potential emergence of variants and COVID.
Also, I have long been suspicious about the effects of tribal affinities on the free flow of information (on many topics). On topics related to the pandemic, there have been major reversals by medical authorities in the past 1 1/2 years that concern me. Some of these relate to the alleged efficacy (and non-efficacy) of mask-wearing, where government mandates were issued in the absence of controlled studies. I am also aware that we have seen very little in the way of data regarding adverse side effects regarding the general population, as well as populations of adolescents and immune-compromised and pregnant individuals. It is also apparent that the misinformation relating to the wearing of masks could be motivated by an inclination to downplay vaccine-related deaths (in order to encourage people to get the vaccines on a nationwide basis).
It is in this context that I am sharing the following materials. I have no medical expertise. I find the following information intriguing. I hope that this information (which has possibly been suppressed) is further developed in the public sphere. Here is the basis for my concerns, a discussion hosted by Brett Weinstein, who has a long history of fearlessly discussing topics that run counter "preferred" public narratives.
The guests suggest that we need an honest conversation regarding use of the the COVID vaccines regarding certain populations where there is natural immunity (children, young teenagers and those who have already had COVID) and where there is alarming data (pregnant women). They also advocate that we badly need honest national dialogue regarding the promising data based on the prophylactic use of repurposed Ivermectin.
Here are two key points made during this deeply engaging discussion:
Point 1. An ongoing course of Ivermectin, long-shown to be a safe drug, is fantastically effective in protecting people from COVID. Brett notes that he and his wife Heather were not vaccinated, but have chosen to use Ivermectin prophylactically. Brett and the guests argue that where a safe alternative to the vaccines is available, this information should be available. The guests are convinced, based on discussed evidence, that Ivermectin is a potentially a "miracle drug" that should be widely repurposed and made available to the public. They are gravely concerned that discussions regarding Ivermectin have been suppressed on the Internet, for social and financial motives they discuss.
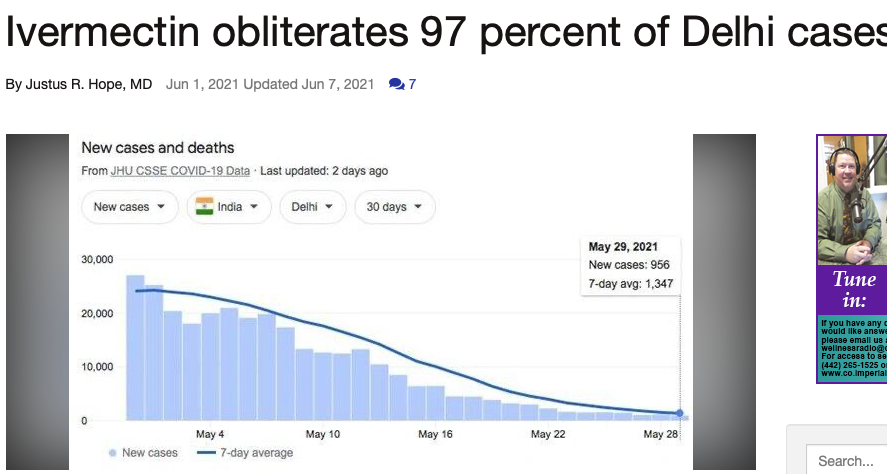
Today, I spotted these graphs regarding Ivermectin usage in India. I cannot vouch for the accuracy of the information in this June 1, 2021 article by Justus R. Hope, a doctor, but it is eye-popping and compels me to know more:
Another excerpt from this article:
A 97% decline in Delhi cases with Ivermectin is decisive - period. It represents the last word in an epic struggle to save lives and preserve human rights. This graph symbolizes the victory of reason over corruption, good over evil, and right over wrong. It is as significant as David’s victory over Goliath. It is an absolute vindication of Ivermectin and early outpatient treatment. It is a clear refutation of the WHO, FDA, NIH, and CDC's policies of "wait at home until you turn blue" before you get treatment.
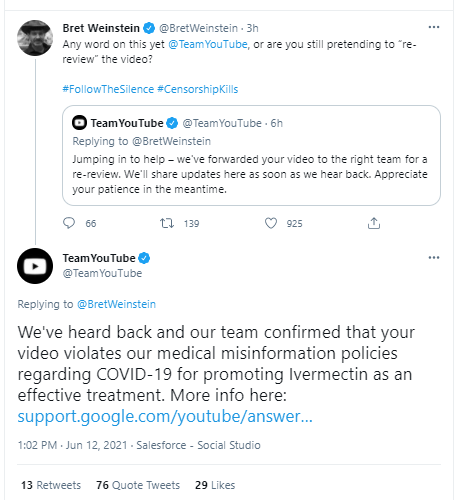
Point 2. On the vaccine side, the guests express concern that there are significant adverse side-effects to the COVID vaccines that are not being discussed widely. In fact, the information is being suppressed, the group strongly suggests, because it doesn't fit the ongoing narrative that the COVID vaccines are "safe." Further, the data regarding adverse side effects is not systematically being collected, much less discussed. The conversation suggests that the VAERS database (voluntary reports) significantly under-reports incidents. Data suggest that the rate of deaths so far from the COVID vaccines in the U.S. might be in the range of 5,000-20,000, the lower end which is greater than the number of deaths from all other vaccines in the U.S. over the past 70 years. For further information on this point, consider Steve Kirsch's recent article at TrialSiteNews, where you will see many details on which he based his concerns in the above video: "Should You Get Vaccinated." The guests also argue that silicon valley is actively suppressing youtube videos and other information. Adverse vaccine-related bloodwork seems to resemble the bloodwork of those who have COVID. The biggest alarm here, the guests agree, is the lack of an alarm.
Here are a few excerpts:
However, based on what I now know about the vaccine side effects, current COVID rates, and the success rate of early treatment protocols, the answer I would give today to anyone asking me for advice as to whether to take any of the current vaccines would be, “Just say NO.”
The current vaccines are particularly contraindicated if you have already been infected with COVID or are under age 20. For these people, I would say “NO! NO! NO!”
In this article, I will explain what I have learned since I was vaccinated that totally changed my mind. You will learn how these vaccines work and the shortcuts that led to the mistakes that were made. You will understand why there are so many side effects and why these are so varied and why they usually happen within 30 days of vaccination. You will understand why kids are having heart issues (for which there is no treatment), and temporarily losing their sight, and ability to talk. You will understand why as many as 3% may be severely disabled by the vaccine.
What I find deeply disturbing is the lack of transparency on how dangerous the current COVID vaccines are. Healthy people could end up dead or permanently disabled at a rate that is “off the charts” compared with any other vaccine in our history. Look at the death report in our government’s official Vaccine Adverse Event Reporting System (VAERS) summarized in the tweet below. This is the most deadly vaccine we’ve ever made by a long shot. That’s why they have to give you incentives to get vaccinated. They need to vaccinate everyone BEFORE people read this article or watch this video of Dr. Peter McCullough explaining clearly why the current COVID vaccines are unsafe and completely unnecessary for our children.
82% miscarriage rate in first 20 weeks (10% is the normal rate). It is baffling that the CDC says the vaccine is safe for pregnant women when it is so clear that this is not the case. For example, one our family friends is a victim of this. She miscarried at 25 weeks and is having an abortion on 6/9/21. She had her first shot 7 weeks ago, and her second shot 4 weeks ago. The baby had severe bleeding of the brain and other disfigurements. Her gynecologist had never seen anything like that before in her life. They called in a specialist who said it was probably a genetic defect (because everyone buys into the narrative that the vaccine is safe it is always ruled out as a possible cause). No VAERS report. No CDC report. Yet the doctors I’ve talked to say that it is over 99% certain it was the vaccine. The family doesn’t want an autopsy for fear that their daughter will find out it was the vaccine. This is a perfect example of how these horrible side effects just never get reported anywhere.
I invite you to listen to the detailed conversation in the video above. I'm writing this as I watch the live discussion. I will update with more after I finish viewing the entire video . . .
[June 12 2021 two updates]
I love this exchange between Steve Kirsch and hundreds of Youtube Subscribers who told him that they appreciated his passion and his message but warned him that his manners were rude and that he was getting in the way of his own message.
Here, for instance, are the powers granted to a 13-year-old child by the state of Washington. Minors age 13 and up are entitled to admit themselves for inpatientand outpatient mental health treatment without parental consent. Health insurers are forbidden from disclosing to the insured parents’ sensitive medical information of minor children—such as that regarding “gender dysphoria [and] gender affirming care.” Minors aged 13 to 18 can withhold mental health records from parents for “sensitive” conditions, which include both “gender dysphoria” and “gender-affirming care.” Insurers in Washington must cover a wide array of “gender-affirming treatments” from tracheal shaves to double mastectomies.
Put these together, and a seventh grader could be entitled to embark on “gender affirming care”—which may include anything from a provider using the child’s name and pronouns to the kid preparing to receive a course of hormones—without her parents’ permission, against her parents’ wishes, covered by her parents’ insurance, and with the parents kept in the dark by insurance companies and medical providers.
This is a detailed, well-researched article that will surprise and shock many families who thought that youth shelters only had relevant for children from broken homes.
Hello, I invite you to subscribe to Dangerous Intersection by entering your email below. You will have the option to receive emails notifying you of new posts once per week or more often.

 Fascinating. So what is it, at bottom, to call someone "mentally ill? Is it essentially name calling? We are surrounded highly functional people who periodically and temporarily seem highly dysfunctional in specific ways. We have been cobbled together by natural selection, living Rube Goldberg machines, we are also equipped with sophisticated built-in PR departments that make it seem like we are more purposeful, more functional than we actually are. Further, Randolph Nesse has made a strong case that many "mental illnesses" are adaptive. What does it help use a global stamp of "mentally ill"?
Fascinating. So what is it, at bottom, to call someone "mentally ill? Is it essentially name calling? We are surrounded highly functional people who periodically and temporarily seem highly dysfunctional in specific ways. We have been cobbled together by natural selection, living Rube Goldberg machines, we are also equipped with sophisticated built-in PR departments that make it seem like we are more purposeful, more functional than we actually are. Further, Randolph Nesse has made a strong case that many "mental illnesses" are adaptive. What does it help use a global stamp of "mentally ill"?