
CNN Uses Cancel Culture Tactics to Attempt to Prevent Vivek Ramaswamy from Saying Obviously True Things
Why do I have almost no respect for corporate media? Here is a recent example of how they function. CNN is trying to dictate that you are not adult enough to hear Ramaswamy's opinions that conflict its preferred narratives and make up your own mind. This is despite the fact that everything Ramaswamy is working so hard to say is established uncontroverted fact. This is corporate media cancel culture at work, motivated by their obeisance to the federal security state. Such shameful behavior by the CNN host.
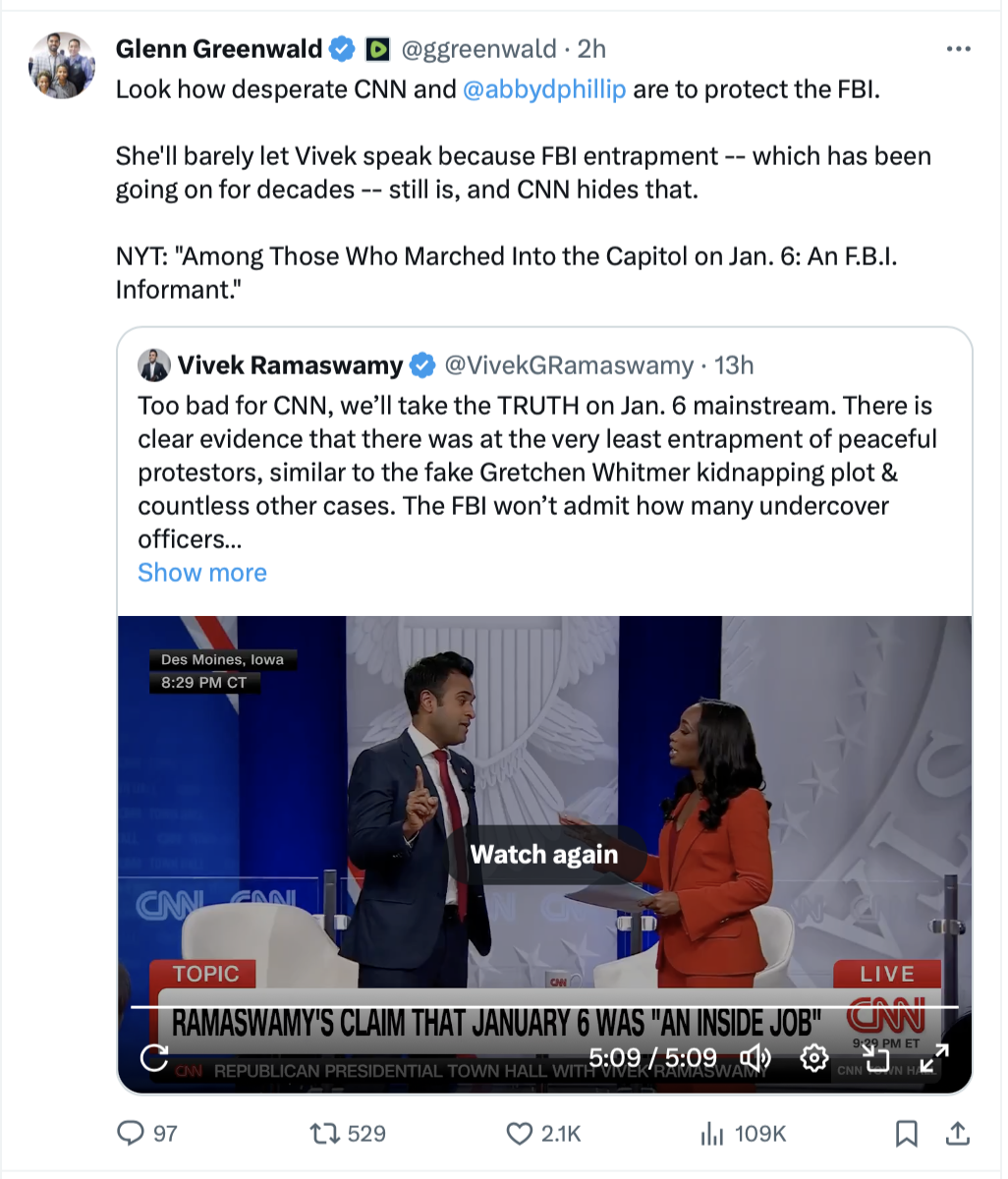
https://twitter.com/ggreenwald/status/1735306093322977484




