I subscribe to evolutionary biologist Colin Wright's new Substack Newsletter, Reality's Last Stand. In his most recent article, "Intersex Is Not as Common as Red Hair," Wright deals with a claim commonly heard from LGBTQ+ activists, the claim that 1.7% of people have intersex conditions, supposedly making it as common as having red hair. Most activists make this claim without any ill-intent. They want to show that intersex conditions are common and the people with these conditions should not be seen as abnormal. The "facts" touted by the activists, however, don't add up.
Many LGBTQ+ activists get their information from a book titled Sexing the Body, by Anne Fausto-Sterling (2000), who got her number from a study asking people to physically describe "idea" males and "ideal" females. For example,
Their “ideal female” has two X chromosomes, functional ovaries that result in normal feminizing puberty, intact oviducts attached to a functional uterus, cervix, and vaginal canal. This ideal female must also have labia minora and majora present, and a clitoris that ranges between 0.20 and 0.85 cm in length at birth.
These "ideal" definitions fails because they include "many conditions that cannot be considered intersex in any clinically relevant sense." The central error was to equate “differences of sexual development” (DSDs) with “intersex.” To illustrate Wright referred to a chart of Fausto-Sterling's data (that was created by Twitter user @zeno001):
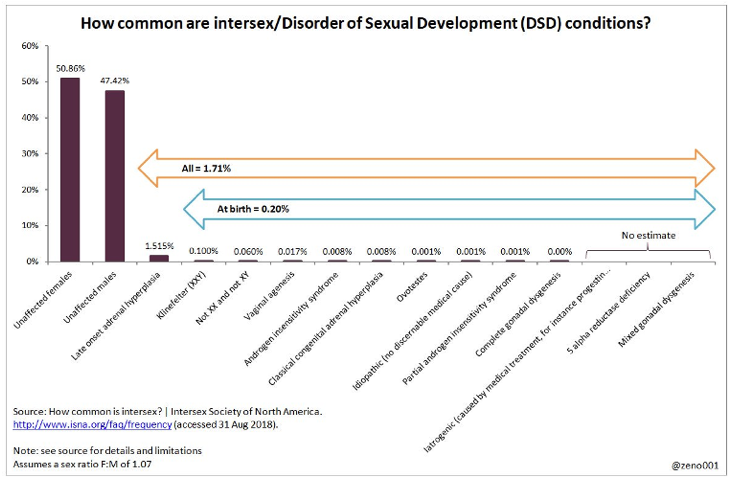
Using this data, Wright points out how misleading the 1.7% claim is.
. . . 88% of Fausto-Sterling’s 1.7% figure is taken up by one condition: late-onset adrenal hyperplasia (LOCAH). These individuals have completely normal male or female genitalia at birth that align with their sex chromosomes. The sex of these individuals is not ambiguous, so to label LOCAH as an intersex condition is a far cry from what most people and clinicians conceptually envision the term to capture.
The next most prevalent DSD on Fausto-Sterling’s list iclude any chromosomal deviations from classical XX and XY (e.g. Klinefelter syndrome, Turner syndrome, etc.). However, these conditions do not result in ambiguous genitalia and therefore cannot be considered intersex in any clinically relevant sense. . . . .
Lastly, vaginal agenesis, the next most common DSD on the list, is not generally considered an intersex condition, as girls with this condition are genotypically XX, possess perfectly normal ovaries, and can even become pregnant and birth their own children following vaginoplasty. They are unambiguously female.
When these common DSDs are removed, and intersex conditions are more precisely defined as “conditions in which chromosomal sex is inconsistent with phenotypic sex, or in which the phenotype is not classifiable as either male or female,” Fausto-Sterling’s 1.7% figure drops dramatically. According to Sax, “Applying this more precise definition, the true prevalence of intersex is seen to be about 0.018%, almost 100 times lower than Fausto-Sterling's estimate of 1.7%.”
With Wright's facts-first approach, the 1.7% claim commonly touted by activists bears no resemblance to reality. As Wright reassures readers, this overstated statistic has no bearing on our duty to treat all intersex people as fully human. They are due the same kindness and respect as any other person. That should never be an issue for anyone, of course.